The data around modern-day colorectal cancer (CRC) screening programs present a remarkable clinical success story. Large-scale randomized controlled trials demonstrate that proactive screening via sigmoidoscopy or colonoscopy lowers CRC incidence by roughly 20% and reduces mortality rate by 26%.(1) By detecting precancerous polyps early and catching tumors at an early stage, screening programs undeniably change patient trajectories. However, for those on the diagnostic side of the tissue sample, this clinical success comes with a notable operational load.
This operational burden is further compounded by two other global trends. The world is witnessing a sharp rise in early-onset CRC cases among adults under the age of 50.(2) Simultaneously, the global pathology workforce is experiencing a significant reduction due to a wave of retirements and recruitment gaps.(3)
The equation is simple but demanding. Biopsy volumes are rising with fewer and fewer specialists available to review them. To maintain diagnostic standards and ensure patient safety, the pathology analysis workflow needs scalable, intelligent tools that support and streamline pathologists' clinical decision-making.
Overcoming interobserver variability and volume challenges in GI pathology
While a clinic might see only a handful of patients a day, standard laboratory protocols require cutting multiple structural levels from every biopsy block. As a result, a single day of routine colonoscopies quickly multiplies into hundreds of slides requiring diagnostic review by a pathologist.(4, 5) At the microscope, each specimen requires a detailed field-by-field review, which, under ideal circumstances, is carried out with deep, uninterrupted focus.
Yet, the chronic staff shortages and increasing sample volumes in modern pathology laboratories point in the opposite direction, forcing clinicians to manage higher case volumes with fewer cognitive breaks. Moreover, traditional histology sample analysis is fundamentally subjective, and heavy workloads and fatigue only amplify this inherent margin for error, making inter- and intra-observer variability a persistent challenge.
The nuances in interpretation show up across daily pathology workflows, particularly when navigating borderline cases, like:
-
Pinpointing the exact boundary between low-grade and high-grade dysplasia in fragmented polyps(6)
-
Meticulously counting tumor buds or poorly differentiated clusters by hand(6)
-
Manually estimating the tumor-stroma ratio (TSR)(7)
-
Assessing baseline severity and spatial distribution of active versus chronic inflammation across large mucosal surfaces.
A recent study examining interobserver variability in adenomas with high-grade dysplasia and early colorectal carcinomas validates how difficult borderline histological samples can be to interpret. The study found that pathologists' diagnoses differed in approximately 40% of high-grade dysplastic adenomas and in 53% of early-stage invasive cancers.(8)
This diagnostic discrepancy rarely stems from a lack of skill. Instead, it reflects how complex, borderline visual cues are highly prone to subjective interpretation, especially when analyzing the last slide after a long, intense shift.
At the same time, manual, repetitive quantifications consume a significant share of a pathologist’s time and cognitive capacity. This ultimately limits the ability to focus on the truly ambiguous, complex cases that demand a pathologist’s deep diagnostic expertise.
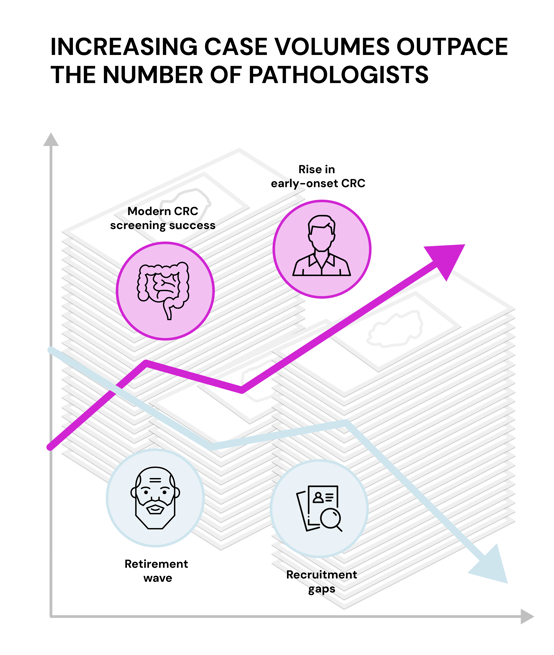
The global data highlights the root cause of the operational burden on pathology laboratories: an intensifying imbalance where rising colorectal cancer (CRC) case volumes are rapidly outpacing a shrinking workforce of pathologists.
Accelerating colon biopsy workflows with AI
While whole-slide imaging (WSI) was a vital first step, digitizing glass slides is not enough to balance the operational load as colonoscopy and sigmoidoscopy biopsy volumes continue to rise. To truly relieve the increasing strain on laboratories, digital GI pathology must evolve from displaying pixels on a monitor to an AI-driven workflow. This switch enables automatic pre-classification of tissue, cell counting, and flagging of areas of interest before the pathologist even opens the case at the start of their shift, sparing them more time to focus on the ambiguous, complex samples.
When AI is used to analyze colon biopsy samples, it is designed to run quietly in the background. It tirelessly and meticulously assists with histology sample analysis, such as carcinoma identification, dysplasia grading, and inflammation scoring. The algorithm prescreens slides to highlight specific tissue structures and areas of interest, providing an immediate starting point for clinical review and seamlessly integrating into the workflow. It generates highly detailed, pixel-level visual overlays that drill down to cell-level architecture, helping pathologists instantly identify the context.
From a laboratory standpoint, the technology helps optimize the broader workflow from end to end. By identifying suspicious morphological features early in the pipeline, the system supports worklist triage and prioritizes the case list so that potential urgent findings surface first. Finally, once the results review is complete, the quantitative data and findings are imported directly into the final report interface, eliminating the need for manual transcription. This reduces daily administrative fatigue and the risk of errors in handheld data transfer.
When AI-powered image analysis takes over the heavy lifting of routine tissue sorting and counting, the practical benefits extend well beyond the laboratory bench to stabilize the entire care pathway. Within the pathology lab, this approach holds the potential to reduce turnaround times and mitigate daily cognitive fatigue. For gastroenterology and oncology teams, it provides consistent, structured data to assist clinical decision-making. Ultimately, the patient benefits from more accurate diagnoses and shorter wait times.
Conclusion
As the volumes of sigmoidoscopy and colonoscopy biopsies continues to climb, integrating AI tools into GI pathology workflows ensures that high-throughput laboratory speed does not come at the cost of diagnostic precision. By handling the highly repetitive aspects of slide analysis and accelerating the analysis process, AI tools act as an extension of the pathologist's eye, enabling them to deliver consistent, precise answers to patients faster and support continued clinical success in the GI specialty.
Interested in seeing how AI-assisted workflows translate to the screen?
Explore our current selection of clinical pathology solutions or reach out to see a live demo of Aiforia® Platform in action.
References:
- Han, C., Wu, F. and Xu, J. (2024) 'Effectiveness of sigmoidoscopy or colonoscopy screening on colorectal cancer incidence and mortality: a systematic review and meta-analysis of randomized controlled trial', Frontiers in Oncology, 14, 1364923. doi:10.3389/fonc.2024.1364923.
- Aldhaleei, W.A., Wallace, M.B. and Bhagavathula, A.S. (2024) 'Trends and age–period–cohort effect on the incidence of early-onset colorectal cancer (20–44 years) from 1990 to 2021 in the United States', Cancers, 16(16), 2883. doi:10.3390/cancers16162883.
- Walsh, E. and Orsi, N.M. (2024) 'The current troubled state of the global pathology workforce: a concise review', Diagnostic Pathology, 19(1), 163. doi:10.1186/s13000-024-01590-2.
- Public Health England. (2021, January 21). Bowel cancer screening: pathology guidance on reporting lesions. https://www.gov.uk/government/publications/bowel-cancer-screening-reporting-lesions/bowel-cancer-screening-guidance-on-reporting-lesions (sited on June 17th 2026)
- Graham, S., Minhas, F., Bilal, M., Ali, M., Tsang, Y. W., Eastwood, M., Wahab, N., Jahanifar, M., Hero, E., Dodd, K., Sahota, H., Wu, S., Lu, W., Azam, A., Benes, K., Nimir, M., Hewitt, K., Bhalerao, A., Robinson, A., ... Rajpoot, N. (2023). Screening of normal endoscopic large bowel biopsies with interpretable graph learning: a retrospective study. Gut, 72(9), 1709-1721. https://doi.org/10.1136/gutjnl-2023-329512
- Lugli, A., Kirsch, R., Ajioka, Y. et al. (2017) 'Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016', Modern Pathology, 30(9), pp. 1299–1311. doi:10.1038/modpathol.2017.46
- van Pelt, G.W., Kjær-Frifeldt, S., van Krieken, J.H.J.M., Al Dieri, R., Morreau, H., Tollenaar, R.A.E.M., Sørensen, F.B. and Mesker, W.E. (2018) 'Scoring the tumor-stroma ratio in colon cancer: procedure and recommendations', Virchows Archiv, 473(4), pp. 405–412. doi:10.1007/s00428-018-2408-z.
- Smits, L.J.H., Vink-Börger, E., van Lijnschoten, G., Focke-Snieders, I., van der Post, R.S., Tuynman, J.B., van Grieken, N.C.T. and Nagtegaal, I.D. (2022) 'Diagnostic variability in the histopathological assessment of advanced colorectal adenomas and early colorectal cancer in a screening population', Histopathology, 80(5), pp. 790–798. doi:10.1111/his.14601.